| Current Emergency Medicine, ISSN 0000-0000 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, Curr Emerg Med and Elmer Press Inc |
| Journal website https://cem.elmerpub.com |
Original Article
Volume 1, July 2026, e3

Clinical Presentation of Vena Cava Syndrome in the Oncologic Intensive Care Unit: A Case Series
Anibal Cortes-Bravoa, b, c ![]() , Angel Fabian Leon-Chavezb, c, h
, Angel Fabian Leon-Chavezb, c, h ![]() , Abel Yurialdy Espinoza-Riosa, d
, Abel Yurialdy Espinoza-Riosa, d ![]() , Carlos Hernan Calderon-Francob, c, e, f
, Carlos Hernan Calderon-Francob, c, e, f ![]() , Katherine Rocio Torresg
, Katherine Rocio Torresg ![]()
aCritical Care Unit, National Cancer Institute, Bogota, Colombia
bInternal Medicine, Subred Centro-oriente Santa Clara Hospital, Bogota, Colombia
cDepartment of Medicine, El Bosque University, Bogota, Colombia
dCritical Care Unit, Subred Centro Oriente, Bogota, Colombia
eDepartment of Cardiology, San Ignacio Hospital, Bogota, Colombia
fDepartment of Medicine, Pontificia Universidad Javeriana, Bogota, Colombia
gDepartment of Medicine, Medicine School, Universidad Militar Nueva Granada, Bogota, Colombia
hCorresponding Author: Angel Fabian Leon-Chavez, Internal Medicine, Subred Centro-oriente Santa Clara Hospital, Bogota, Colombia
Manuscript submitted February 3, 2026, accepted April 13, 2026, published online July 17, 2026
Short title: Clinical Presentation of VCS in the Oncologic ICU
doi: https://doi.org/10.14740/cem3
| Abstract | ▴Top |
Background: Vena cava syndrome (VCS), particularly superior vena cava syndrome (SVCS), is caused by obstruction of venous return to the right atrium and may represent an oncologic emergency depending on symptom severity, most often due to malignant tumors compressing or invading the vena cava. SVCS is prevalent among patients in oncologic intensive care unit (ICU), with significant clinical implications and high mortality.
Methods: We conducted a descriptive case series including 19 patients diagnosed clinically and radiologically with VCS, treated in the Oncologic ICU of the National Cancer Institute in Bogota between 2022 and 2025. We analyzed clinical, oncologic, imaging, and outcome variables, including Yu severity classification, Kishi intervention score, thrombotic events, critical complications, anticoagulant use, and mortality.
Results: The mean age was 46.5 years, and 57.9% were male. Solid tumors predominated (57.9%), with non-Hodgkin lymphoma as the most common cause (36.8%), followed by lung carcinoma (15.8%). Fourteen patients (73.7%) had SVCS, and five (26.3%) had inferior vena cava syndrome (IVCS). Respiratory symptoms, mainly dyspnea, were present in 89.5% of the patients. Collateral circulation was observed in 84.2% of patients, predominantly via the azygos–hemiazygos system. According to Yu classification, 12 patients (63.2%) were grade 4, whereas seven (36.8%) were distributed across grades 1–3, and 13 patients (68.4%) had a Kishi score > 4. Thrombosis occurred in 52.6%, with 63.6% of these patients’ receiving anticoagulation. Ventilatory failure developed in 79.8%, and 36.8% experienced acute kidney injury (mostly Kidney Disease: Improving Global Outcomes (KDIGO) stage 3). Overall mortality was 57.9%.
Conclusions: In this ICU cohort, malignant VCS—predominantly SVCS—was associated with frequent organ dysfunction and high in-hospital mortality. Early identification, clinical stratification, and targeted intervention are essential to reduce mortality. The findings underscore the need for specific management protocols in oncologic ICUs to improve outcomes.
Keywords: Vena cava syndrome; Oncologic emergencies; Intensive care; Thrombosis; Lung cancer; Non-Hodgkin lymphoma; Hospital mortality
| Introduction | ▴Top |
Superior vena cava syndrome (SVCS) is caused by obstruction of venous blood flow, leading to a broad spectrum of clinical signs and symptoms [1]. The clinical presentation of SVCS is highly variable, ranging from asymptomatic cases to conditions that pose an imminent threat to life [2]. This variability is attributable to the narrowing of the vessel lumen, which impedes the return of blood from the head, neck, and both upper and lower extremities, thereby compromising the Cavo atrial junction. As such, SVCS is considered a clinically significant condition that may require urgent intervention in severe presentations [3, 4].
This condition can affect both the superior vena cava (SVC) and the inferior vena cava (IVC) [5], although it predominantly involves the SVC. This predominance is attributable to the anatomical location of the SVC, which is closely associated with vital structures such as the heart, pulmonary artery, main bronchi, and the cervical and mediastinal lymphatic chains, all of which facilitate extrinsic compression. Such compression compromises the vessel’s diameter, which typically ranges from 7 to 8.5 cm, and disrupts the normal pressure gradient of approximately 3 mm Hg towards the right atrium [2, 3].
Elevations in this gradient result in congestion of the veins in the neck, brachial region, and upper thorax, thereby producing the characteristic symptoms [2]. In approximately 60% of cases, these symptoms are secondary to primary or metastatic tumors, followed by thrombosis related to intravascular devices such as venous catheters and pacemakers (30–40%), as well as aortic aneurysms, substernal thyroid hypertrophy, and granulomatous diseases such as tuberculosis [2, 6, 7].
The first description of SVCS was provided by William Hunter in 1757, who documented that obstructions at this level—whether due to extrinsic compression or thrombosis—resulted in a characteristic clinical presentation [3]. This presentation is primarily defined by the presence of neck edema (82%), arm edema (68%), respiratory symptoms such as dyspnea (66%) and cough (50%), as well as collateral circulation in the thorax (38%) [8–10]. Cutaneous manifestations, including cervical ecchymosis and plethora, are also frequently observed.
Notably, these symptoms tend to improve with the upright position [11]. Nevertheless, it is important to emphasize that the resultant pressure overload can precipitate cerebral edema, thereby significantly increasing the risk of coma and brain injury [4].
Clinical severity should be documented using validated clinical classifications, because manifestations range from asymptomatic disease to life-threatening compromise and correlate with the degree of venous obstruction [1].
In this context, the Kishi score is employed to assess neurological, oropharyngeal, and facial symptoms, as well as venous distension [4, 11], to determine the necessity for interventional therapy when the score exceeds 4 [1, 2].
It is important to assess the clinical presentation using the Yu severity system, which classifies cases from asymptomatic to fatal based on clinical signs and the extent of systemic involvement [5, 11]. Moderately severe cases account for the highest incidence (50%), followed by mild clinical presentations (25%), while fatal cases represent only a very small proportion of new cases (1%) [3, 4, 11].
Among the etiologies, cancer is the primary cause of SVC obstruction [2, 4, 11]. The tumors most commonly associated with SVCS are non-small cell lung cancer (50%) and small cell lung cancer (22%), followed by lymphomas (12%)—including non-Hodgkin lymphoma and primary mediastinal lymphoma—as well as breast cancer (9%) and metastatic tumors (9%) [9, 11]. These malignancies account for approximately 90% of SVCS cases related to cancer [2, 6]. Nevertheless, benign etiologies such as intravascular devices, pacemakers, mediastinal diseases, and iatrogenic causes represent up to 30% of all cases of SVCS [3]. Therefore, establishing an accurate etiological diagnosis is fundamental in the management of this condition [2].
There are multiple diagnostic options available, including clinical assessment, chest radiography, computed tomography (CT) of the neck and chest, magnetic resonance imaging (MRI), and venography. These are noninvasive modalities that can be performed with low levels of contrast [2, 6]. In many patients, chest radiographs are abnormal (84%), revealing mediastinal involvement (64%) and pleural effusion (26%) [7, 8]. However, contrast-enhanced CT is particularly valuable, as it allows for precise evaluation of the size and cause of the obstruction, the presence of associated thrombosis, and the identification of collateral vessels. This imaging modality is highly sensitive (92%) and specific (96%) for SVCS [1, 7], making it the most relevant study for providing a comprehensive overview of the clinical situation and guiding potential interventions [3, 8]. It is important to highlight the role of retrograde collateral drainage due to increased pressure in the vena cava, most commonly towards the azygos vein, followed by the hemiazygos system, the mammary veins, and the epigastric vessels [1, 4].
Treatment is categorized into supportive therapy and definitive therapy, with priority given to stabilizing the critical condition over establishing a pathological diagnosis [6]. The severity of the syndrome determines the therapeutic approach [11]. Among general supportive measures, elevating the head of the bed to 30 degrees is recommended to decrease orthostatic pressure in the head and neck [1], along with the use of diuretics to manage edema [1, 4, 8].
In patients presenting with grade 1 or 2 SVCS, therapeutic interventions are primarily directed towards addressing the underlying etiology of the disease [5]. For those with grade 3 or 4 SVCS, thrombolytic therapy or anticoagulation has been proposed as potential treatment options [2, 5]. Nevertheless, in the context of malignancy, management must be tailored to include glucocorticoids, fibrinolytic therapy, and chemotherapy [9]. Notably, lymphomas demonstrate high sensitivity to both corticosteroids and chemotherapy [12], with dexamethasone, prednisone, and prednisolone representing the corticosteroids with the most significant therapeutic response [4]. Conversely, solid tumors—particularly those of pulmonary origin—are highly responsive to radiotherapy [8, 13]. Thus, precise identification of the underlying etiology of SVCS is essential to prevent recurrent obstruction [6, 9]. Current evidence supports radiotherapy and chemotherapy as the mainstays of treatment for this clinical syndrome, with specific recommendations varying according to the literature [1].
Endovascular stent placement has been considered as a last-resort therapeutic option when there is inadequate response to anticoagulation, chemotherapy, and radiotherapy [5, 11, 12]. However, this technique often yields suboptimal outcomes in oncologic patients due to the heterogeneity of underlying malignancies, with post-stent complication rates ranging from 3% to 8%. These complications include severe vascular injury, episodes of re-thrombosis, and device migration [2, 9]. Open surgical management should be reserved exclusively for benign conditions, as anatomical alterations and tumor recurrence in malignant cases significantly diminish surgical success rates [12]. Furthermore, premature intervention may precipitate additional complications [3, 12]. It is also noteworthy that the median survival for patients with severe SVCS admitted to intensive care unit (ICU) in the context of oncologic emergencies ranges from 1.5 to 9.5 months [8, 14].
SVCS represents a high-severity, high-priority condition in intensive care units, particularly among oncologic and hemato-oncologic patients. Therefore, it is crucial to provide optimal management, especially in tumor-related cases, where clinical presentation and severity grading guide therapeutic decisions [1, 3, 4, 8, 9]. The present study aims to describe the clinical characteristics of patients with malignant VCS, predominantly SVCS, admitted to the Oncology ICU at the National Cancer Institute in Bogota, Colombia (INC). We hypothesized that, within this ICU cohort, malignant VCS would present predominantly as severe disease, with frequent organ dysfunction and high in-hospital mortality.
| Materials and Methods | ▴Top |
Study design
This is a descriptive case series study involving 19 patients diagnosed with malignant vena cava syndrome (VCS).
Study population
Nineteen medical records of patients identified through institutional diagnostic coding and confirmed by manual review of the electronic medical record, imaging findings, and established diagnostic classifications who were admitted to the oncology ICU at the National Cancer Institute in Bogota, Colombia, between 2022 and 2025, were reviewed.
Inclusion and exclusion criteria
Included in the study were adult patients (over 18 years of age) with both clinical and radiological diagnoses of malignant VCS (superior or inferior) requiring management in the ICU. Pediatric patients and those receiving care in the palliative care unit were excluded.
Study variables
The following variables were analyzed: sociodemographic data (age and sex); tumor type (distinguishing between hematologic and solid malignancies, with further characterization by pathology); location of the affected segment of the vena cava; presence of other oncologic emergencies such as tumor lysis syndrome or malignant hypercalcemia; involvement of collateral venous pathways; cardinal presenting symptom of VCS; associated symptoms; degree of vena cava obstruction according to the Yu classification; treatment classification according to Kishi; imaging findings and dimensions of extrinsic lesions; presence of associated thrombosis; use of anticoagulant therapy; description of critical complications such as ventilatory failure (including type of ventilatory failure), presence of renal injury and its classification according to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines; Eastern Cooperative Oncology Group (ECOG) performance status to determine oncologic disease status; and mortality during critical illness.
Data collection
Data were collected systematically and comprehensively through an exhaustive manual review of the electronic medical record, including clinical notes, laboratory results, and imaging studies, to gather information on the proposed variables.
A database was constructed in Excel, characterizing each variable in accordance with the guidelines established by the institutional ethics and research committee.
Data analysis
A descriptive analysis was performed for categorical and continuous variables. Categorical variables were summarized using absolute and relative frequencies. Continuous variables were described using exploratory distribution assessment and descriptive summary measures. Statistical analysis was conducted using the JAMOVI software package.
Ethics committee/Institutional Review Board (IRB) approval
This study was reviewed and approved by the Institutional Ethics and Research Committee of the National Cancer Institute of Bogota, in accordance with national regulations governing health research. Given the retrospective and observational nature of the study, the requirement for informed consent was waived by the committee.
Ethical compliance with human study
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and in compliance with applicable national regulations governing health research. As an observational, retrospective study based on document review, no experiments involving human participants were performed. Patient confidentiality and data anonymization were ensured at all stages of the research process.
| Results | ▴Top |
A total of 19 cases of VCS were analyzed. The mean age of the population was 46.5 years. Regarding sex distribution, VCS was more prevalent in males (11 cases, 57.9%). Solid tumors were the most common underlying malignancy, accounting for 11 cases (57.9%). However, when analyzing specific oncologic diagnoses, seven cases of VCS were associated with non-Hodgkin lymphoma (36.8%), followed by lung carcinoma with three cases (15.8%). The remaining diagnoses each accounted for a single case (5.3%) (Table 1).
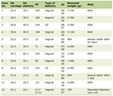 Click to view | Table 1. Clinical Characteristics, Severity, Complications, and Outcomes (N = 19) |
The most frequent clinical presentation was SVCS, observed in 14 cases (73.7%), while inferior vena cava syndrome (IVCS) occurred in five patients (26.3%). Seven patients developed oncologic complications consistent with tumor lysis syndrome (36.8%), and one case presented with malignant hypercalcemia (5.3%). Collateral circulation involvement was assessed, revealing that 11 cases (57.9%) exhibited compromise of the azygos–hemiazygos venous system, four cases (21.1%) involved the internal thoracic collateral circulation, and three cases (15.8%) affected the vertebral and paravertebral circulation. One case (5.3%) involved the lateral thoracic collateral system.
Regarding cardinal symptoms, respiratory manifestations predominated, occurring in 17 cases (89.5%), while two cases (10.5%) presented with neurological alterations secondary to VCS. Among respiratory symptoms, dyspnea was the principal determinant, occurring in 14 cases (73.7%). Additional symptoms included delirium in one case (5.3%) and altered level of consciousness due to stupor in one case (5.3%).
Evaluation using the Kishi score revealed that 13 cases (68.4%) had a score > 4, indicating the need for urgent interventional evaluation. According to the Yu classification, 12 patients (63.2%) were grade 4, whereas the remaining seven patients (36.8%) were distributed across grades 1–3. Regarding tomographic findings of the tumor lesions causing VCS, lymph node conglomerates were identified in seven cases (36.8%), and cervical masses were present in six cases (31.6%). The mean volume of these tumor lesions was 95.3 mm3.
The occurrence of thrombotic episodes was observed in 10 cases (52.6%). Among patients with thrombosis, four presented with thrombosis of the SVC (44.4%), and three had thrombosis of the jugular vein (33.3%). Other documented sites of thrombosis included the femoral vein and intracardiac thrombi. Of the patients experiencing thrombotic episodes, seven patients received anticoagulation therapy (63.6%): four with dalteparin (21.1%) and three with heparin (33.3%). In two patients, thrombotic events were managed with the placement of a vena cava filter (22.2%).
Echocardiographic assessment of left ventricular ejection fraction (LVEF) and tricuspid annular plane systolic excursion (TAPSE) was performed, documenting a median LVEF of 57% (interquartile range (IQR): 28.5–63.5) and a mean TAPSE of 23.6 mm.
Regarding complications, 15 patients developed ventilatory failure (79.8%), with ventilatory failure due to shock (type IV) in six patients (40%), followed by hypoxemic ventilatory failure (type I) in five patients (33.3%). Seven patients developed acute kidney injury (36.8%), of which six cases corresponded to KDIGO stage 3 acute kidney injury (85.7%). The oncologic stage of the patients was assessed using the ECOG performance status, revealing that seven cases had an ECOG score of 4 (36.8%). The mortality rate in the studied group was 11 out of 19 cases (57.9%) (Table 1).
The continuous variables analyzed included age, tumor mass volume causing VCS, LVEF, and TAPSE. Figure 1 provides an exploratory visual representation of the distribution of these variables. Given the small sample size, these plots are presented for descriptive purposes.
 Click for large image | Figure 1. Distribution plots of age, tumor lesion volume, LVEF, and TAPSE. LVEF and TAPSE are shown together with their respective violin and box plots, illustrating the descriptive distribution of each variable. LVEF: left ventricular ejection fraction; TAPSE: tricuspid annular plane systolic excursion. |
| Discussion | ▴Top |
VCS, most characteristically SVCS, may represent an oncologic emergency when severe symptoms or organ dysfunction are present, particularly in ICUs [3, 4, 9]. In this case series, 19 patients admitted to an oncologic ICU were described, with a high proportion of cases associated with hematologic malignancies, especially non-Hodgkin lymphoma (36.8%), followed by solid tumors such as lung carcinoma (15.8%). These findings are consistent with the literature, where malignant neoplasms account for up to 90% of SVCS cases, with non-small cell lung cancer being the most frequent, followed by lymphomas and metastatic tumors [15–17].
In this study, 73.7% of cases corresponded to SVCS, confirming the predominance of this anatomical location in oncologic populations due to the proximity of the SVC to mediastinal structures frequently affected by tumor masses or lymph node conglomerates. This pattern aligns with the description by Wilson et al, who reported that up to 85% of adult SVCS cases are due to malignant processes, mainly lung cancer and lymphomas [9, 18–20].
The mean age of 46.5 years contrasts with previous studies, where the median age is usually between 60 and 65 years [15, 11, 21]. This difference may be explained by the predominance of hematologic tumors in this cohort, especially non-Hodgkin lymphoma (36.8%), which more commonly affects young adults. This finding underscores the importance of considering histological type in the epidemiological profile of VCS, as hematologic tumors tend to be more sensitive to medical therapy (chemotherapy and steroids), which modifies the therapeutic approach compared to solid tumors [1, 22].
Respiratory symptoms as the cardinal clinical presentation in 89.5% of cases reinforce their diagnostic utility, with dyspnea being the predominant symptom. This finding is consistent with the pathophysiology of SVCS, where venous obstruction leads to retrograde venous hypertension, edema, and respiratory compromise [5, 16, 21, 23, 24]. The high frequency of collateral circulation towards the azygos–hemiazygos system (57.9%) represents an expected physiological adaptation, with important diagnostic value when observed in contrast-enhanced imaging as an indirect marker of chronic or subacute obstruction [4, 25, 24].
The use of the Kishi score and Yu classification allowed descriptive categorization of clinical severity. In this series, 12 of 19 patients (63.2%) were classified as Yu grade 4, and 13 of 19 (68.4%) had a Kishi score > 4, which is consistent with the severe profile expected in an oncologic ICU. Given the descriptive design and the absence of a comparator group, these findings should be interpreted as severity descriptors within this cohort rather than as predictors of outcome.
The high rate of thrombotic events (52.6%) highlights the need for early evaluation of associated vascular complications, particularly in the presence of intravascular catheters or advanced disease. This prevalence exceeds that reported in international series, where thrombotic events range between 20–40% [11, 12], which could be explained by the selection of critically ill patients or delays in initial oncologic intervention. Furthermore, intracavitary thrombosis and involvement of territories such as the jugular or femoral veins suggest significant disease extension [4, 5, 17].
Regarding therapy, most patients received anticoagulant treatment, and in some cases, a vena cava filter was used. Although the use of filters is reserved for cases with contraindications to anticoagulation or recurrent events, their use in this cohort reflects the clinical severity and multidisciplinary approach in the critical care context. Published series and reviews recommend their selective use, based on hemorrhagic risk and thrombotic progression [3, 26, 27].
Associated complications such as ventilatory failure (79.8%) and acute kidney injury (36.8%) are consistent with the literature describing VCS as a systemic condition compromising multiple organs [28, 29]. Notably, more than 85% of patients with acute kidney injury presented with KDIGO stage 3, which has been described as a strong predictor of mortality in the context of sepsis or multiorgan failure [28, 29].
The observed mortality rate (57.9%) in this series evidences the high lethality of VCS in critical oncologic settings, being higher than that reported in outpatient or general hospitalized populations. Previous studies describe mortality rates between 30% and 45% in patients with advanced solid tumors and central vascular involvement [13, 30]. This outcome is consistent with the finding of an ECOG ≥ 3 in many cases, a condition that predicts poor prognosis [5, 8, 14].
Etiological, clinical, and evolutionary differences must be considered when designing specific care pathways, considering the particularities of hematologic versus solid tumors. In addition, the relatively young age of the cohort and the predominance of non-Hodgkin lymphoma are observations that may reflect the institutional referral pattern and warrant confirmation in larger series. Future research should focus on standardizing integrated management algorithms to improve survival and quality of life in this vulnerable population.
Limitations
This study has important limitations. It was a single-center descriptive case series with a small sample size, without a control group or longitudinal follow-up, so causal inferences cannot be made. In addition, the cohort reflects only patients admitted to the oncologic ICU; therefore, the findings should not be extrapolated to all patients with VCS treated at the institution.
Conclusions
The present study describes VCS in critically ill oncologic patients, with non-Hodgkin lymphoma emerging as the predominant etiology. Complications such as thrombosis, ventilatory failure, and acute kidney injury were frequent in this ICU cohort.
The Yu and Kishi classifications were useful to describe clinical severity within this series. Multicenter studies are warranted to validate these findings and to promote integrated management strategies aimed at optimizing the prognosis of these patients in oncologic ICUs.
Acknowledgments
The authors wish to acknowledge the medical, nursing, and administrative staff of the Oncologic ICU at the National Cancer Institute of Bogota for their support in patient care and for facilitating access to the clinical information required for the completion of this study.
Financial Disclosure
The authors declare that no specific funding was received from public, commercial, or non-profit funding agencies for the conduct of this study.
Conflict of Interest
The authors declare that they have no conflicts of interest related to this work.
Informed Consent
Informed consent was not obtained, as this study is a retrospective review of medical records, involved no direct patient intervention, and exclusively used anonymized data.
Author Contributions
Study conception and design: all authors. Data acquisition: all authors. Data analysis and interpretation: all authors. Manuscript drafting: all authors. Critical revision for important intellectual content: all authors. Final approval of the submitted version: all authors accept responsibility for the content of the manuscript and approve its final version.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
| References | ▴Top |
- Shah RP, Bolaji O, Duhan S, Ariaga AC, Keisham B, Paul T, Aljaroudi W, et al. Superior vena cava syndrome: an umbrella review. Cureus. 2023;15(7):e42227.
doi pubmed - Klein-Weigel PF, Elitok S, Ruttloff A, Reinhold S, Nielitz J, Steindl J, Hillner B, et al. Superior vena cava syndrome. Vasa. 2020;49(6):437-448.
doi pubmed - Patriarcheas V, Grammoustianou M, Ptohis N, Thanou I, Kostis M, Gkiozos I, Charpidou A, et al. Malignant superior vena cava syndrome: state of the art. Cureus. 2022;14(1):e20924.
doi pubmed - Lepper PM, Ott SR, Hoppe H, Schumann C, Stammberger U, Bugalho A, Frese S, et al. Superior vena cava syndrome in thoracic malignancies. Respir Care. 2011;56(5):653-666.
doi pubmed - Yu JB, Wilson LD, Detterbeck FC. Superior vena cava syndrome—a proposed classification system and algorithm for management. J Thorac Oncol. 2008;3(8):811-814.
doi pubmed - Jafari A, Rezaei-Tavirani M, Salimi M, Tavakkol R, Jafari Z. Oncological emergencies from pathophysiology and diagnosis to treatment: a narrative review. Soc Work Public Health. 2020;35(8):689-709.
doi pubmed - Straka C, Ying J, Kong FM, Willey CD, Kaminski J, Kim DW. Review of evolving etiologies, implications and treatment strategies for the superior vena cava syndrome. Springerplus. 2016;5:229.
doi pubmed - Wan JF, Bezjak A. Superior vena cava syndrome. Hematol Oncol Clin North Am. 2010;24(3):501-513.
doi pubmed - Wilson LD, Detterbeck FC, Yahalom J. Clinical practice. Superior vena cava syndrome with malignant causes. N Engl J Med. 2007;356(18):1862-1869.
doi pubmed - Higdon ML, Atkinson CJ, Lawrence KV. Oncologic emergencies: recognition and initial management. Am Fam Physician. 2018;97(11):741-748.
pubmed - Quencer KB. Superior vena cava syndrome: etiologies, manifestations, and treatments. Semin Intervent Radiol. 2022;39(3):292-303.
doi pubmed - Sen I, Kalra M, Gloviczki P. Interventions for superior vena cava syndrome. J Cardiovasc Surg (Torino). 2022;63(6):674-681.
doi pubmed - Ahs. Clinical practice guideline RT-005 palliative radiotherapy: superior vena cava obstruction, dyspnea, and hemoptysis [Internet]. 2016. Available from: institutional clinical practice guideline source.
- Spring J, Munshi L. Oncologic emergencies: traditional and contemporary. Crit Care Clin. 2021;37(1):85-103.
doi pubmed - Rowell NP, Gleeson FV. Steroids, radiotherapy, chemotherapy and stents for superior vena caval obstruction in carcinoma of the bronchus: a systematic review. Clin Oncol (R Coll Radiol). 2002;14(5):338-351.
doi pubmed - Guhlich M, Maag TE, Droge LH, El Shafie RA, Hille A, Donath S, Schirmer MA, et al. Symptom relief, prognostic factors, and outcome in patients receiving urgent radiation therapy for superior vena cava syndrome : A single-center retrospective analysis of 21 years' practice. Strahlenther Onkol. 2022;198(12):1072-1081.
doi pubmed - Mir T, Uddin M, Shafi O, Qureshi W, Kaur J, Zghouzi M, Lohia P, et al. Thrombotic superior vena cava syndrome: a national emergency department database study. J Thromb Thrombolysis. 2022;53(2):372-379.
doi pubmed - Ellison MB, Statler A, Henrickson RE, Graff J, Sloyer D, Abbas Khan MA, Hayanga HK, et al. Iatrogenic superior vena cava syndrome after cardiopulmonary bypass diagnosed by intraoperative echocardiography. Case Rep Anesthesiol. 2020;2020:8813065.
doi pubmed - Aung EY, Khan M, Williams N, Raja U, Hamady M. Endovascular Stenting in Superior Vena Cava Syndrome: A Systematic Review and Meta-analysis. Cardiovasc Intervent Radiol. 2022;45(9):1236-1254.
doi pubmed - Azizi AH, Shafi I, Shah N, Rosenfield K, Schainfeld R, Sista A, Bashir R. Superior vena cava syndrome. JACC Cardiovasc Interv. 2020;13(24):2896-2910.
doi pubmed - Hinton J, Cerra-Franco A, Shiue K, Shea L, Aaron V, Billows G, Al-Hader A, et al. Superior vena cava syndrome in a patient with locally advanced lung cancer with good response to definitive chemoradiation: a case report. J Med Case Rep. 2018;12(1):301.
doi pubmed - Yellin A, Rosen A, Reichert N, Lieberman Y. Superior vena cava syndrome. The myth—the facts. Am Rev Respir Dis. 1990;141(5 Pt 1):1114-1118.
doi pubmed - Koegelenberg CF, Bolliger CT, Plekker D, Wright CA, Brundyn K, Louw M, Schubert P, et al. Diagnostic yield and safety of ultrasound-assisted biopsies in superior vena cava syndrome. Eur Respir J. 2009;33(6):1389-1395.
doi pubmed - Morin S, Grateau A, Reuter D, de Kerviler E, de Margerie-Mellon C, de Bazelaire C, Zafrani L, et al. Management of superior vena cava syndrome in critically ill cancer patients. Support Care Cancer. 2018;26(2):521-528.
doi pubmed - Markman M. Diagnosis and management of superior vena cava syndrome. Cleve Clin J Med. 1999;66(1):59-61.
doi pubmed - Ratzon R, Tamir S, Friehmann T, Livneh N, Dudnik E, Rozental A, Hamburger-Avnery O, et al. Thrombosis, anticoagulation and outcomes in malignant superior vena cava syndrome. J Thromb Thrombolysis. 2019;47(1):121-128.
doi pubmed - Sun M, Chen X, Li H, Zhang X, Wang X, Zheng R, Li G, et al. Clinical analysis of 48 cases of malignant superior vena cava syndrome. World J Surg Oncol. 2021;19(1):185.
doi pubmed - Ponti A, Saltiel S, Rotzinger DC, Qanadli SD. Insights into endovascular management of superior vena cava obstructions. Front Cardiovasc Med. 2021;8:765798.
doi pubmed - Akin Y, Cagli K, Okten RS, Keles T, Golbasi Z. Pacemaker-associated superior vena cava syndrome: Role of contrast echocardiography. Echocardiography. 2022;39(4):647-653.
doi pubmed - Tunc M, Sazak H, Karlilar B, Ulus F, Tastepe I. Coexistence of obstructive sleep apnea and superior vena cava syndromes due to substernal goitre in a patient with respiratory failure: a case report. Iran Red Crescent Med J. 2015;17(5):e18342.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
Current Emergency Medicine is published by Elmer Press Inc.